“In 2017, Nabarro and Tedros competed for the WHO Director-General role. …Tedros’s candidacy was mired in several scandals”
By Stacey Rudin

Last week, in a major departure from months of pro-lockdown messaging, Britain’s envoy to the WHO Dr. David Nabarro called for world leaders to stop locking down their countries and economies as a “primary method” of controlling COVID19. “I want to say it again: we in the World Health Organization do not advocate lockdowns as the primary means of control of this virus,” Dr. Nabarro told The Spectator.
“The only time we believe a lockdown is justified is to buy you time to reorganise, regroup, rebalance your resources, protect your health workers who are exhausted, but by and large, we’d rather not do it.” Dr. Nabarro’s position aligns with the Great Barrington Declaration, of which he spoke favorably, in which 30,000 scientists and public health experts have joined in advocating an immediate return to normal life for those at low risk. Nabarro and the thousands of signees of the Declaration opine that this approach will minimize overall mortality and lessen the disproportionate burden of lockdowns on the working class and underprivileged.
The day after Nabarro made his remarks, WHO director-general Dr. Tedros Adhanom Ghebreyesus flatly contradicted him, declaring that lifting lockdowns would be a recipe for “unnecessary infections, suffering and death.” Tedros claims that herd immunity can only be “safely” achieved through vaccination, a conclusion premised upon the frightening assumption that the development of a safe and effective vaccine is guaranteed, and the dubious premise that natural infections can be held back “as long as it takes” to prepare and distribute the vaccine. However, according to Tedros, there is no other way: “allowing a dangerous virus that we don’t fully understand to run free is simply unethical. It’s not an option.”
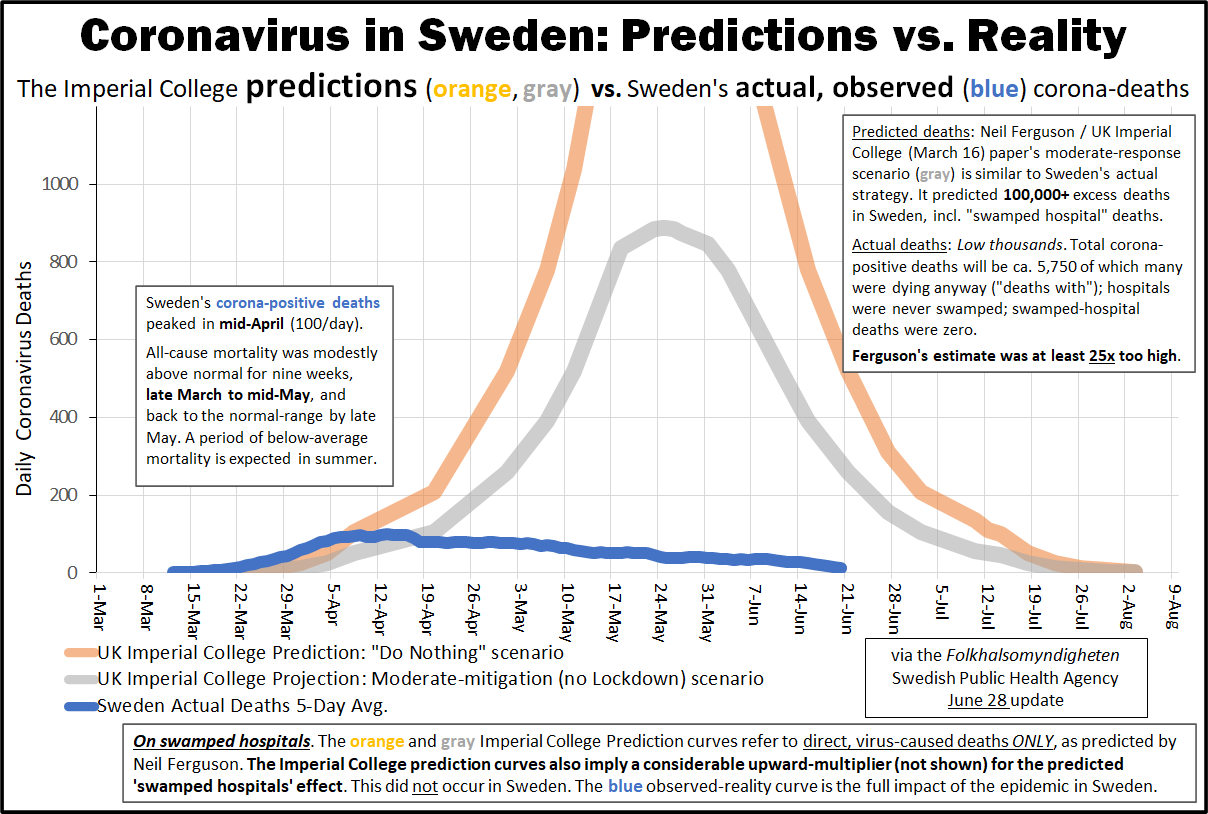
It’s difficult to reconcile this stance with the data from states and nations which did not lock down for COVID19. For example, Swedish all-cause mortality is on average for 2020 — incredibly, the nation had higher per-capita mortality just five years ago, in a year in which there was no pandemic. This undeniable, easily-verifiable fact is shocking in light of the decimation of world economies on the premise of “stopping” a “highly deadly” pathogen. Far from “unethical,” allowing the virus to “run free” produced a much better result than tight lockdowns such as those imposed in Argentina and Peru — yet Tedros is ignoring this. The question is: why?
The China-Paved Path to WHO Director-General
In 2017, Nabarro and Tedros competed for the WHO Director-General role. For the first time, the position was filled by a direct vote of the member-states, and not by the WHO executive board. Tedros’s candidacy was mired in several scandals. Ethiopians and concerned global citizens pleaded with the countries voting in the election to reject Tedros because he was a representative of a repressive political regime who had helped to build and maintain a surveillance state with a total lack of government transparency. Critics pointed out that Tedros was “comfortable with the secrecy of autocratic states”— a characteristic that could wreak havoc on the world if he assumed a position of power within the WHO.
Tedros also received criticism for his role in covering up cholera epidemics while he was Ethiopia’s Health Minister from 2005 until 2012. Tedros summarily dismissed the complaint, raised by one of Nabarro’s advisers, likening it to James B. Comey’s reopening of the investigation into Hillary Clinton’s private email server just days before the 2016 presidential election. He also attributed racial and elitist motives to his accuser, claiming “Dr. Nabarro’s backers have a ‘typical colonial mind-set aimed at winning at any cost and discrediting a candidate from a developing country.’” [Big words for a creature of Bill Gates.]
However, the undisputed facts depict a Health Minister who is doing one of two things: grossly neglecting cholera testing, or intentionally prioritizing his nation’s economy over protecting people from cholera. Tedros claimed that outbreaks of what he called “acute watery diarrhea” in 2006, 2009, and 2011 were not cholera, although he could not produce a test ruling out the deadly pathogen, and neighboring Somalia and Kenya disclosed cholera as the cause of their own simultaneous outbreaks.
Tedros claimed that testing in his country was “too difficult,” but this was belied by the fact that outside experts were able to test and find the cholera bacteria in stool samples. Testing for cholera bacteria is simple and takes less than two days. It is hard to fathom why outside experts and other countries would be able to test while the Ethiopian government could not.
Cholera can kill a person in as little as five hours. News of cholera outbreaks can have a quick and devastating impact on a country’s economy, so African nations sometimes fail to declare cholera emergencies even when they know for a fact that they have one. During the 2006 outbreak, for example, Ethiopia “did not share the results of lab tests since [the outbreak started]” because “it can mean some serious economic losses,especially in terms of international trade and tourism,” said Kebba O. Jaiteh, emergency officer in Ethiopia with the WHO.
During earlier outbreaks of cholera in Ethiopia (or “acute watery diarrhea,” depending on who you believe), The Guardian and The Washington Post investigated and reported that Ethiopian officials “were pressuring aid agencies to avoid using the word ‘cholera’ and not to report the number of people affected.” Research by Human Rights Watch found that the Ethiopian government “was pressuring its health workers to avoid any mention of cholera, which could damage the country’s image and deter tourists.” Despite this accumulation of evidence, Tedros stood by his denial, preventing aid from being delivered to Ethiopians: the UN cannot act without permission and a declaration of an outbreak.
Vaccines are also unavailable when a country fails to declare a cholera outbreak, so Tedros refused his countrymen this option even when their neighbors in Somalia and Kenya received it. This seems to have escaped the notice of Dr. Seth Berkley, CEO of Gavi, the vaccine alliance, who praised Tedros’s “commitment” to human health and vaccination: “Tedros’s commitment to immunization is clear . . . His work with Gavi as Ethiopia’s health minister helped boost the proportion of children reached by vaccines from less than half to more than two-thirds.” Other defenders of Tedros included former CDC director Tom Frieden, who was appointed by Barack Obama to head the Agency for Toxic Substances and Disease Registry. Frieden praised Tedros as “an excellent choice to lead the WHO,” and today vocally agrees with Tedros on lockdowns, masks, and social distancing.
Tedros’s strongest and most important backer throughout these controversies was not an individual, but a government: China. As an opinion writer in the Indian press described it, “China propped Tedros.” American apathy in the public health arena had allowed China to “colonize” global health:
“One reason that Tedros has gotten away with so much brazen cronyism is that America pays little to no attention to global public health, save pouring in money as a sugar daddy . . . China started a scheme for global health colonisation and won because America didn’t think it was important enough. The Chinese leveraged their investments across Africa to force the African Union to back Tedros, [and] also got Pakistan to withdraw its candidate who was opposing him,sources say . . . India’s diplomatic credentials helped in covering up Tedros’ shady past and the fact his main backer was a Communist dictatorship.”
“I’ve Got Your Back, and You’ve Got Mine”: Tedros Backs the Chinese COVID19 “Supression” Strategy
Fast-forward to the COVID19 epidemic. In early 2020, Tedros went to great lengths to congratulate China on its response to the “novel coronavirus.” On January 30, the WHO issued a statement effusively praising China’s response, highlighting the Chinese government’s “commitment to transparency” and efforts to “investigate” and “contain” the outbreak. The statement declares that China’s novel “lockdown” strategy — wherein dictator Xi Jinping welded people inside their apartments in the name of “disease control” — are “good not only for that country but also for the rest of the world.” Tedros followed this up with a tweet: “China is actually setting a new standard for outbreak response.” During this time period, hundreds of thousands of social media posts later traced to China praised the lockdown, and criticized and ridiculed world leaders who failed to follow suit.
The WHO’s resounding praise of China continued into February 2020, when it convened a “Global Research and Innovation Forum” on the novel coronavirus to study “the origin of the virus, natural history, transmission, diagnosis, infection prevention and control,” among other things. On February 24, the group’s Joint Mission held a press conference to report on its findings, during which it declared, “there is no question that China’s bold approach to the rapid spread of this new respiratory pathogen has changed the course of what was a rapidly-escalating and continues to be deadly epidemic.” The stated basis for this unequivocal declaration on the effectiveness of lockdowns was as follows:
“And there’s a couple of other graphics . . . here’s the outbreak that happened in the whole country on the bottom. Here’s what the outbreak looked like outside of Hubei. Here are the areas of Hubei outside of Wuhan. And then the last one is Wuhan. And you can see this is a much flatter curve than the others. And that’s what happens when you have an aggressive action that changes the shape that you would expect from an infectious disease outbreak.
This is extremely important for China, but it’s extremely important for the rest of the world, where this virus you’ve seen in the last few days is taking advantage to explode in certain settings. And it wasn’t easy because what I didn’t mention on this slide is every one of these lines represent a huge decision by policy makers and politicians in this country and leaders to actually change the shape with big measures such as, you know, the suspension of travel, the stay-at-home advisories, and other incredibly difficult measures; to make decisions about, but also to get a population to follow. And that’s why, again, the role of the individual here in China is so important as well.”
The Joint Mission’s conclusion that China’s actions “worked” is a perfect depiction of the classic logical fallacy post hoc, ergo propter hoc: Latin for “it happened after, so it was caused by.” While it is indeed possible that a “more flat” curve in Wuhan could be attributed to government mandates, there are equal or greater possibilities: one, that testing protocols differed; two, that China simply witnessed the natural course of this “novel” pathogen. The latter is particularly likely since there was no baseline with which to compare the proffered epicurves.
It should be obvious that the mere issuance of government mandates does not automatically mean they were effective — this is particularly true here, since the global scientific community had previously considered and rejected large-scale quarantines as a method for controlling epidemics. Respiratory viruses never spread evenly throughout countries, provinces, or states, so it was nothing short of reckless to conclude that the noted variance in spread — which again, could be nothing but a recording error due to testing aberrations — was due to anything but natural factors. It was criminal to summarily conclude on this evidence that the Chinese government’s draconian actions led to a “favorable outcome,” and then use that patentily illogical conclusion to sell lockdowns to the rest of the world. But that’s just what the WHO did.
“China didn’t approach this new virus with an old strategy for one disease or another disease. It developed its own approach to a new disease and extraordinarily has turned around this disease with strategies most of the world didn’t think would work . . . What China has demonstrated is, you have to do this. If you do it, you can save lives and prevent thousands of cases of what is a very difficult disease.”
The Joint Mission repeated this assertion — “lockdowns work, they can and do save lives” — in various ways throughout its press conference, recalling to mind the words of a famous propagandist named Joseph Goebbels: “repeat a lie often enough and it becomes the truth.” Research shows that this illusion of truth effect “works just as strongly for known as for unknown items, suggesting that prior knowledge won’t prevent repetition from swaying our judgements of plausibility.” Our parents never heard of lockdown, and understood and accepted that humans sadly cannot “stop” a highly contagious infectious disease like the flu — even with a vaccine — yet suddenly most of the planet was behaving as if this were not only a reasonable mission, but something for which it was rational and desirable to sacrifice social lives, relationships, smiles, businesses, and educations in service of.
At the helm of the WHO, Tedros undoubtedly played a key role in the creation of this perception. Thanks to the many individual worldwide lockdown experiments, we now know that he was dead wrong: no lockdown was ever needed to “flatten the curve” — in fact, lockdowns spiked the curve. No-lockdown Sweden’s epicurve was much flatter than many areas with tight lockdowns, including New York City, Italy, and Spain. While this may be adequately explained by Hanlon’s Razor, it is very interesting that the Joint Mission took great pains to protect China’s trade and travel interests despite advocating simultaneous lockdowns for other nations:
“And this brings us to what I think is one of the most important recommendations we would make in respect to getting China fully back on its feet after this crisis. The world needs the experience and materials of China to be successful in battling this coronavirus disease. China has the most experience in the world with this disease, and it’s the only country to have turned around serious large-scale outbreaks. But if countries create barriers between themselves and China in terms of travel or trade, it is only going to compromise everyone’s ability to get this done.
And those kinds of measures need to be anything that goes beyond what’s been recommended by the IHR committee, has got to be reassessed, because the risk from China is dropping, and what China has to add to the global response is rapidly rising.”
The human rights community did not share this enthusiasm for China, its draconian lockdown, or its offer to “help” other nations contend with the virus. On February 2, The Guardian published an opinion piece by a human rights advocate outlining the lockdown’s serious human rights violations and opining that the WHO broke its own commitment to “human rights and health” by praising China. The WHO’s commitment reads in part:
“Human rights are universal and inalienable. They apply equally, to all people, everywhere, without distinction. Human Rights standards — to food, health, education, to be free from torture, inhuman or degrading treatment — are also interrelated. The improvement of one right facilitates advancement of the others. Likewise, the deprivation of one right adversely affects the others”
To protect these “universal and inalienable” human rights during a public health emergency, international law requires that restrictions on human rights be based on legality, necessity, proportionality and grounded in evidence. Similarly, the Siracusa Principles — in which the United Nations outlines an overarching international covenant on civil and political rights — state that restrictions on rights and freedoms in the name of public health must be strictly necessary and the least intrusive available to reach their objective:
“In the exercise of his rights and freedoms, everyone shall be subject only to such limitations as are determined by law solely for the purpose of securing due recognition and respect for the rights and freedoms of others and of meeting the just requirements of morality, public order and the general welfare in a democratic society.”
“Lockdown” goes far beyond these basic human rights boundaries. They are proven now to only damage societies — they even worsen COVID19 outcomes. When The Economist analyzed all recorded epidemics since 1960, it concluded that “democracies experience lower mortality rates for epidemic diseases than their non-democratic counterparts.” This finding holds true at all levels of income.
Tedros aligned himself not with democracies and their fundamental principles but with an autocratic dictatorship, the same dictatorship that helped him assume power within the WHO. Together, using logical fallacies and pseudo-science, they betrayed international law governing human rights, the WHO’s own stated principles, and committed crimes against humanity on a massive scale. Should we continue to listen to Tedros, or should we turn to Dr. Nabarro, another qualified expert who — like the thousands who signed the Great Barrington Declaration — urges a return to democratic norms as necessary to minimize human suffering?
“Lockdowns just have one consequence that you must never, ever belittle, and that is making poor people an awful lot poorer. Just look at what’s happened to smallholder farmers all over the world. Look what’s happening to poverty levels. It seems that we may well have a doubling of world poverty by next year.” — Dr. David Nabarro
It is no longer possible to ignore Tedros Adhanom Ghebreyesus’s long history with suppressive autocratic regimes, including China. Whatever the motivation behind his advocacy for continued lockdowns, the data invalidates his position unequivocally. Lockdowns do not save lives — lockdowns kill. The reign of tyranny must end, immediately and forever, with a full restoration of the rights and privileges of each individual citizen to choose what level of risk he or she will accept as a law-abiding member of a functioning, democratic society.
WHO, what, where, and why? We don’t yet have all of the answers, but we do know that the WHO director-general is on the wrong side of the lockdown debate.
Source: AIER



























 Source:
Source: 
{kind=link}
{kind=link}